About
Terms of Use
Privacy Policy
Ophthalmic Medication Table
Patient Name:
Date:
Please separate all drops by at least 5 minutes.
Medication:
Top Color:
Eye:
Right
Left
Both
to right eyelid
to left eyelid
to both eyelids
to incision
Oral
Nasal Spray
Times per day:
Suggest common frequencies
A suggested frequency was filled in. You can edit it.
Add
Print
Cap Color
Medication
Eye
Times per day
Action
The ad below will not print with your drops table.
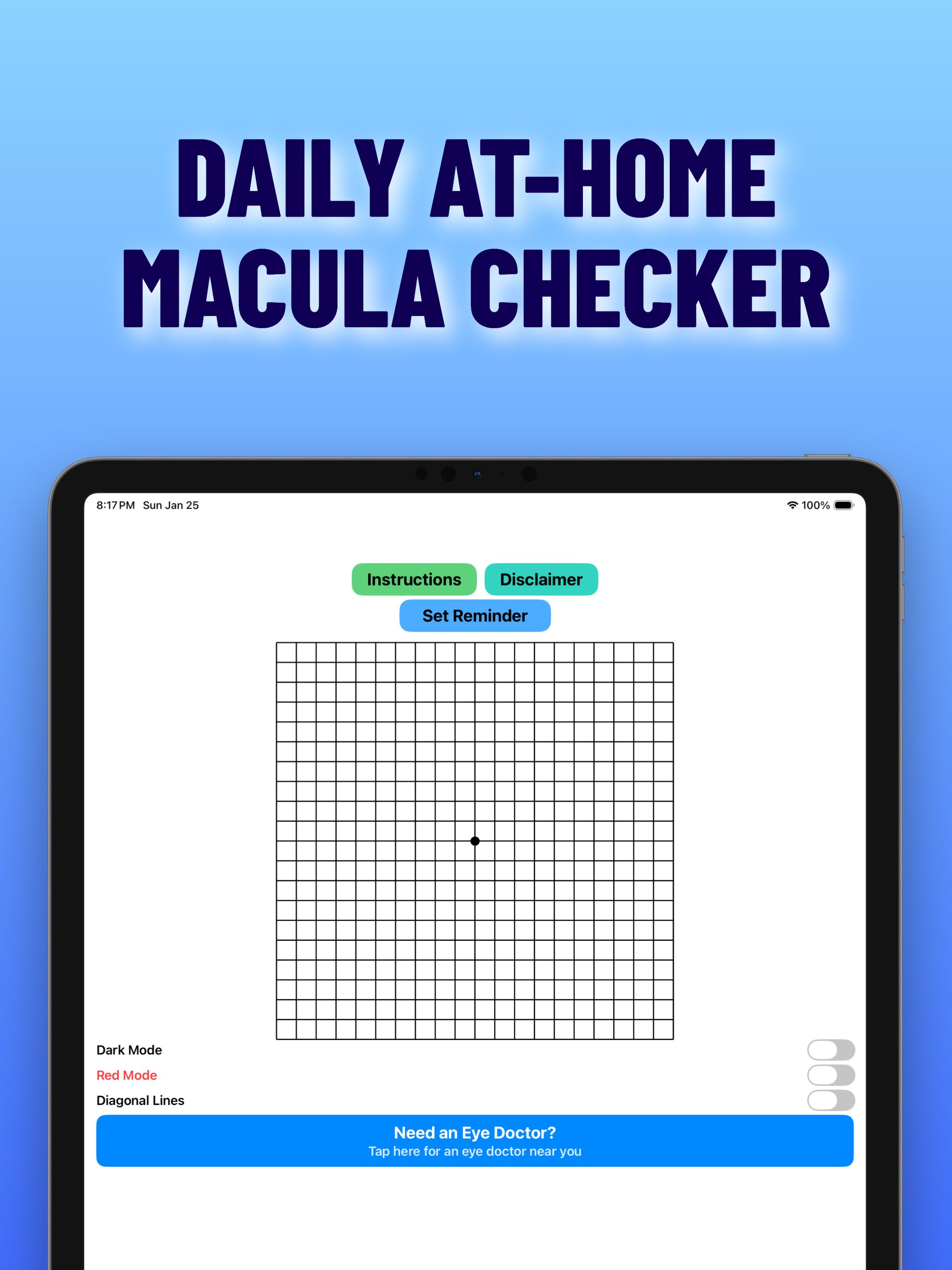
Amsler — an iPhone and iPad app for your patients
Free listing for ophthalmology practices - Don't worry this ad won't print with your drops table.
See Amsler
Get Listed Free
Patient Handouts
This tool is for convenience only and does not provide medical advice. Verify all instructions with a licensed eye care professional. Medication names are for identification only.
×